AI-Powered Medical Scribe for Emergency Medicine
Practice medicine again.
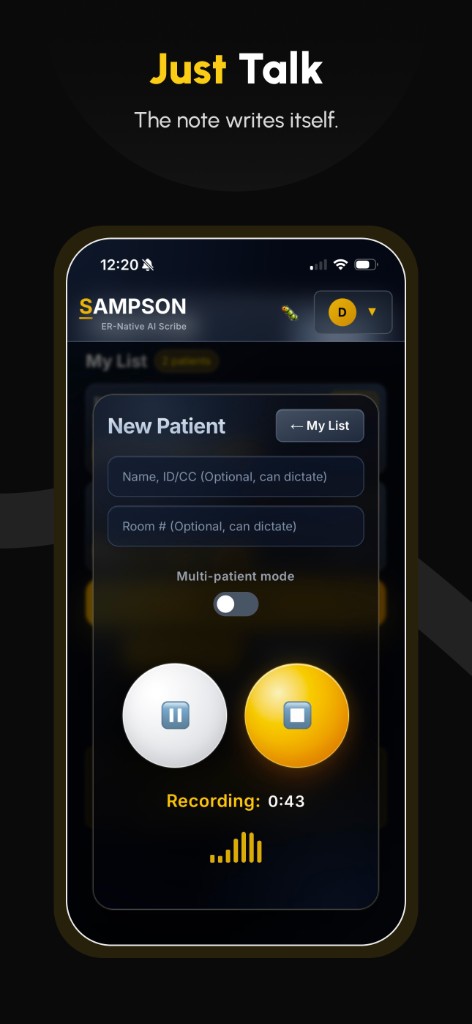
Hit record. Drop your phone in your pocket. Go see your patient like you normally would. Sampson handles the note—complete, billable, defensible, and ready in under a minute.
You didn't spend years in training to spend half your shift dictating.
You made it through years of training and thousands of clinical hours. You can run a resus in your sleep. Somehow the job became 40% data entry.
Your CMG's “solutions” were built by people who've never set foot in a resuscitation bay. We built something different.
How It Works
Three steps. That's it.
Record
Hit record on your phone. See your patient. Sampson listens in the background—even with your screen locked.
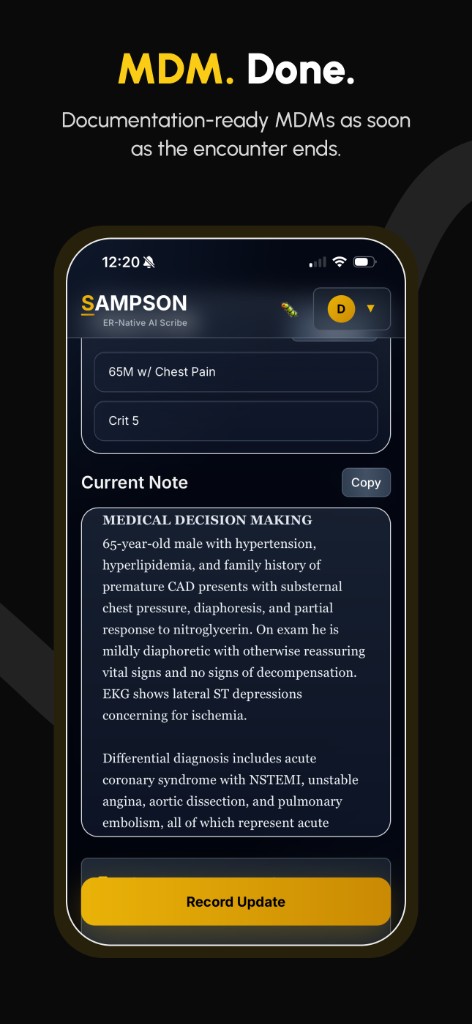
Generate
AI builds the full note: HPI, exam, MDM—structured around 2023 E/M guidelines. Most notes in under a minute.
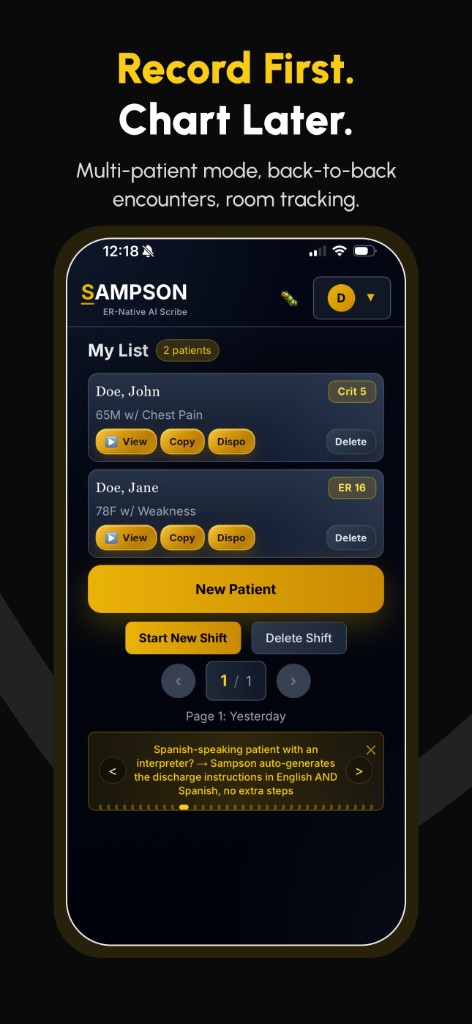
Review & Paste
Copy/paste into your EMR. Read through, adjust if needed. Done before your next patient hits the board.
No templates. No endless clicking. No charting from home.
Accuracy First
Built to get it right.
Most AI scribes are general-purpose tools duct-taped onto medicine. Sampson was designed from the ground up for the emergency department.
Medical-Grade Transcription
Sampson uses advanced transcription software built specifically for medical terminology—because the note is only as good as the transcript it’s built from.
Clinical Context, Not Just Transcription
AI scribes that treat everything said in an encounter as equally true produce notes that don’t reflect clinical reality. Sampson is built to distinguish between what was said and what matters clinically. Patient speculation stays in context. Background conversations stay out. The note reflects your assessment—structured around what you actually found, considered, and decided.
Adjustable Conciseness
A detailed HPI that captures everything the patient said tells a jury you took the time to listen. A tight, focused note means less time spent reviewing before signing. Sampson lets you dial in the level of conciseness—from comprehensive to streamlined—so the documentation matches your style.
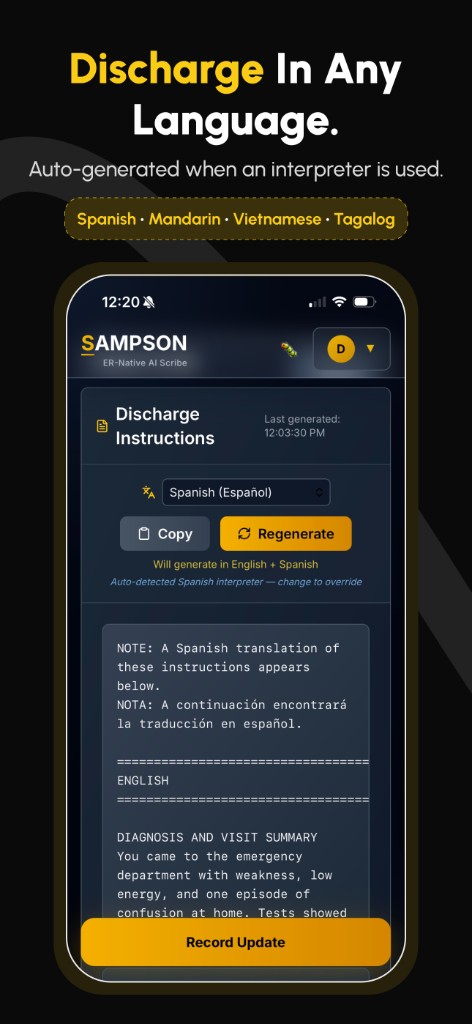
See It In Action
Take Back Control.
Excellent. Profitable. Bulletproof.
Notes that pay today and cover your ass tomorrow.
Medical Excellence
The patient’s note is done before you’ve even entered your orders. Structured, thorough, and clinically precise—notes that will both impress and help your consultants and colleagues.
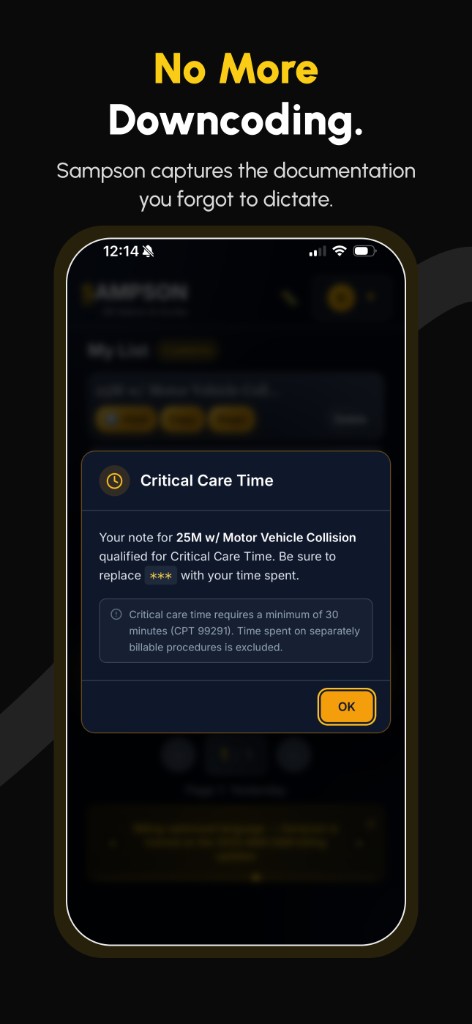
Billing Optimization
You’re already doing complex medicine—you should get paid for it. Sampson captures the MDM you actually performed, built around 2023 E&M guidelines. Stop leaving money on the table.
Medicolegal Defense
Three years from now, when someone pulls your chart, it tells the whole story. What you considered. What you ruled out. Why you made the call. Documentation that has your back.
Real Output
This is what Sampson actually produces.
One section of a complete ED note—generated from a single dictation. Billing-optimized documentation, risk stratification, decision tools, consultant documentation, and a defensible differential. All captured automatically.
1Documents independent historian credit under 2023 E/M guidelines
3Captures independent interpretation of tests to optimize billing credit
5High-risk medication — captures risk category credit
7Timestamped consult — billable + medicolegal
65-year-old male with hypertension and hyperlipidemia presents with chest pain. Reports chest pain that started while at rest, worsened with exertion, and associated with nausea and diaphoresis. History obtained from EMS who served as an independent historian1 who gave full dose aspirin and nitroglycerin and noted stable vitals in the field.
Differential diagnosis includes acute coronary syndrome, aortic dissection, pulmonary embolism, and pneumothorax, all of which pose a threat to life or bodily function2, as well as musculoskeletal chest wall pain and gastroesophageal reflux disease.
I independently interpreted3 the EKG as normal sinus rhythm with anterolateral ST depressions and no STEMI criteria. Troponin was 251 and uptrended to 321 . CBC, CMP, and UA without clinically significant acute findings. I independently interpreted the CXR as no acute findings; radiologist later agreed. I reviewed outpatient echocardiogram dated 08/13/2025 showing EF 55–60%, which informed ED management.4 Patient started on a heparin infusion for NSTEMI, which is a high-risk medication requiring intensive monitoring5. HEART score is 7. Wells PE score is 06. Discussed with hospitalist Dr. Robinson at 06:32 PM7; patient will be admitted for cardiac workup. Discussed with cardiologist Dr. Smith at 05:59 PM who will evaluate the patient and make recommendations. Patient is stable for admission at this time.
At this time, low clinical suspicion for pulmonary embolism based on Wells PE score 08. Low clinical suspicion for pneumothorax based on no respiratory distress and CXR with no acute findings. Low clinical suspicion for aortic dissection based on normal hemodynamics and no ripping/tearing quality. Low clinical suspicion for esophageal rupture based on normal CXR and no history of vomiting/retching.
Admitted to medicine/telemetry.9
2Billing-optimized differential — optimizes billing credit under complexity of problems addressed
4Review of outside records — billing credit for data reviewed
6Validated decision tools — medical necessity and risk billing credit
8Structured reasoning — automatically defends against dangerous and less likely diagnoses
9Clear disposition — closes the clinical loop
Documents independent historian credit under 2023 E/M guidelines
Billing-optimized differential — optimizes billing credit under complexity of problems addressed
Captures independent interpretation of tests to optimize billing credit
Review of outside records — billing credit for data reviewed
High-risk medication — captures risk category credit
Validated decision tools — medical necessity and risk billing credit
Timestamped consult — billable + medicolegal
Structured reasoning — automatically defends against dangerous and less likely diagnoses
Clear disposition — closes the clinical loop
No investors. No corporate overlords.
Just fed-up EM docs.
Sampson was built between patients by emergency physicians who got tired of choosing between finishing charts and getting home to their families.
No venture capital. No health system backing. The big players are coming for this space—Epic, Nuance, your CMG's next contract. Sampson is built for you, not for them.
The Sampson Team
Built by board-certified emergency physicians
Your data stays yours.
We don't screw around with your data. Sampson doesn't feed your notes into a training dataset. Your documentation isn't used to build a general AI model. It isn't sold, shared, or recycled. Ever. Period. The encounter goes in, the note comes out, the data is auto-deleted, and that's the end of it.
We're not building a platform that learns to practice medicine. We're building a tool that helps you document it.
Questions. Fair.
Yes. Fully encrypted in transit and at rest, BAA in place, the whole nine. We don't mess around with patient data.
All of them. Sampson generates the note—you paste it wherever you need it. Epic, Cerner (Oracle Health), Meditech, CPSI, eClinicalWorks, T-System—whatever your shop runs.
Sampson is designed to omit rather than invent — if something wasn't clearly part of the encounter, it doesn't end up in the note. You review and sign every note before it goes in the chart, just like you would with a human scribe. The difference is that Sampson's output is consistent and structured enough that review is a quick scan, not a rewrite.
It's completely free for clinicians right now. We're still finalizing long-term pricing, and clinicians who join early and help shape the product will get a full year of free access.
Sampson doesn't integrate with or connect to your EHR. You record into the app, review the note, and paste it into your chart. There's nothing for IT to install. From your EHR's perspective, you wrote the note.
Because I use this every shift. My documentation, my license, my RVUs. If it didn't work, I'd know first.
Apply for access.
Sampson is available to verified clinicians. Create your account and we'll review it — most applications are reviewed within a day.
Take your time back.
You didn't go into medicine to write notes. Stop letting documentation run your life.
Apply for Access